Research
Group members
Dr Sayka Barry and Dr Federica Begalli (Postdoctoral Fellows); Dr Chung Lim (Clinical Training Fellow), Dr Kesson Magid (Database Manager); Ms Anisha Mistry (PhD student); Mr Solomon Muna (Clinical Fellow); Ms Oniz Suleyman (Senior technician); Dr Nicola Tufton (Clinical Training Fellow). Writing up status: Dr Donato Iacovazzo (Diabetes UK Clinical Training Fellow); Ms Karen Young (MRC Clinical Training Fellow)
Close collaborator: Dr Oliver Haworth (Lecturer)
Selected Past Lab Members
Dr Blerina Kola (Clinical Training Fellow); Dr Chrysanthia Leontiou (PhD student); Dr Craig Stiles (Wellcome Clinical Training Fellow); Dr Daniela Aflorei (Clinical Training Fellow); Dr Edwin Garcia (Postdoctoral Fellow); Dr Francesco Ferrau (Visiting Clinical Fellow); Dr Giampaolo Trivellin (Postdoctoral Fellow); Dr Harvinder Chahal (MRC Clinical Training Fellow); Dr Erika Hubina (Clinical Training Fellow); Dr Ida Pernicova (Clinical Training Fellow); Dr Julia Thomas (Clinical Training Fellow); Dr Laura Hernandez-Ramirez (Clinical Training Fellow); Dr Marton Doleschall (Postdoctoral Fellow); Dr Mirjam Christ-Crain (Clinical Training Fellow); Dr Pam Gabrovska (Database Manager); Dr Serban Radian (Marie Curie Research Fellow); Alejandro Ibanez Costa (Postdoctoral Fellow); Dr Antonia Solomou (Postdoctoral Fellow); Dr Francisca Palou (Clinical Fellow); Dr David Collier and Dr Amy Ronaldson (Database Managers); Tatsuya Komogata (visiting scientist); Dr Sherine Awad (Bioinformatician)
Pituitary and Neuroendocrine Group
Prof Korbonits’ research group concentrates on the etiology and tumorigenic process of familial and sporadic pituitary adenomas. She set up a website for this disease for patients and health care professionals (https://www.qmul.ac.uk/fipa-patients/) and established the International FIPA consortium to study the clinical, genetic and molecular characteristics of these patients. The groups’ major focus concerns the mechanism by which loss-of-function AIP mutations cause particularly aggressive adenomas at a young age, studies centered around the analysis of human samples and new in vivo models of human disease (in collaboration with Carles Gaston-Massuet), including in the fruit fly. In parallel, in vitro assays are helping to complete the cycle of pituitary adenoma variant identification to pathological understanding of disease etiologies.
The group has shown that an AIP mutation (Arg304Stop) that was introduced into the DNA of a resident of Northern Ireland some 2500 years ago helps explain the long history of Irish giants (Figure 1). Their genetic studies, which have established that this founder mutation still survives in this population today (Figure 2) (see further details at: https://www.qmul.ac.uk/fipa-patients/irish-giants/), provides an excellent example of how genetic screening, followed by clinical screening of carrier family members can identify pre-symptomatic patients, leading to earlier diagnosis and more personalized treatment and a better long-term prognosis. These data has now been confirmed in our large cohort (Marques, JCEM, 2020). The group are now investigating a second founder mutation due to replication slippage mechanism (Figure 3) affecting nine families living in three different countries (UK, France and USA) but all originating from a single founder probably in England from several hundred years ago (Figure 4).
 Figure 1. AIP Mutations and Gigantism. First panel. 18th century patient with gigantism due to a mutation of AIP (aryl hydrocarbon receptor interacting protein) beside his twin cousins who also had gigantism, in an etching by John Kay (1742–1826) (National Portrait Gallery, London) (Chahal, NEJM, 2011). Middle panel. Ribbon representation of the crystal structure of human AIP (based on data published in Morgan, PlosOne, 2012 and Linnert, Biomol.NMR Assign., 2012) with the stop mutation from the 18th-century patient marked in red. Right-hand panel. A hand of a 4th-year male medical student (172 cm tall) compared to the tracing of the hand of an Irish patient from the 18th century with gigantism (tracing from Frankom, G; Musgrave, J.H. The Irish giant, 1974, Duckworth, London).
Figure 1. AIP Mutations and Gigantism. First panel. 18th century patient with gigantism due to a mutation of AIP (aryl hydrocarbon receptor interacting protein) beside his twin cousins who also had gigantism, in an etching by John Kay (1742–1826) (National Portrait Gallery, London) (Chahal, NEJM, 2011). Middle panel. Ribbon representation of the crystal structure of human AIP (based on data published in Morgan, PlosOne, 2012 and Linnert, Biomol.NMR Assign., 2012) with the stop mutation from the 18th-century patient marked in red. Right-hand panel. A hand of a 4th-year male medical student (172 cm tall) compared to the tracing of the hand of an Irish patient from the 18th century with gigantism (tracing from Frankom, G; Musgrave, J.H. The Irish giant, 1974, Duckworth, London).
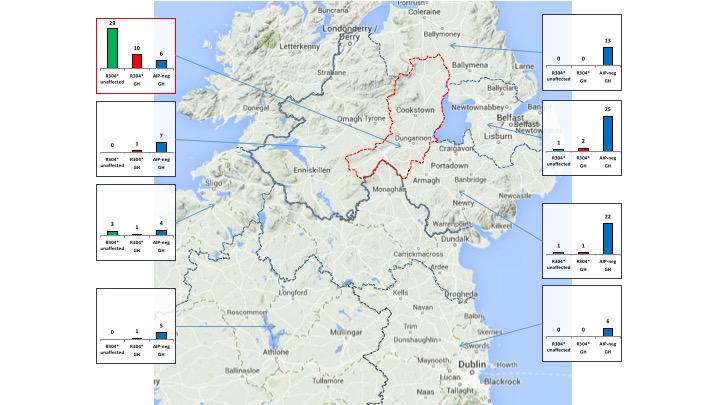
Figure 2. In Ireland, the highest geographical concentration of the Irish Giant AIP R304* allele is found in Mid Ulster (red dotted line). R304* carriers: unaffected (green columns) and patients with somatotrophinomas (red). AIPmut-negative patients with somatotrophinomas (AIP-neg GH, blue columns). Only current residents of Ireland were screened. R304*-positive patients with other pituitary adenoma types (n=5) are not shown. Each small graph summarizes data from the underlying region. From Radian S et al, Human Mutation 2017.
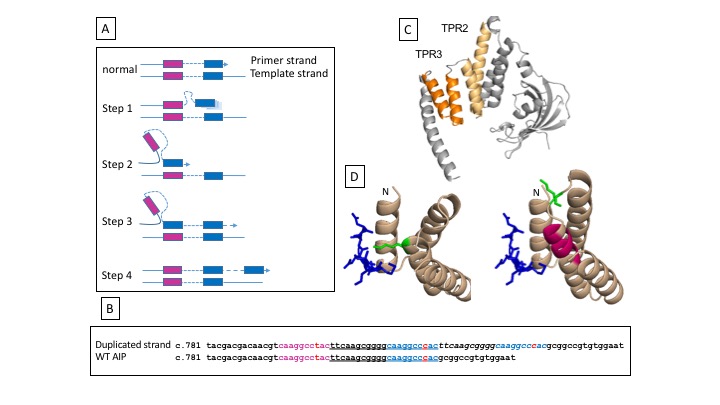
Figure 3. In-frame seven amino acid duplication of aryl hydrocarbon receptor protein (AIP) reduces protein stability and interaction with Heat Shock Protein 90 (HSP90)
A) Schematic of the suggested replication slippage mechanism creating the c.805_825dup, p.F269_H275duplication. The purple and blue colorings match the sequences in B). During DNA replication, the primer strand containing the newly synthesized second repeat transiently dissociates from the template, slips backwards and then re-associates at the first short direct repeat of the template strand, resulting in a misaligned configuration. Continued DNA synthesis is envisaged to lead to the insertion of the intervening sequence and the second direct repeat, resulting in the duplicated allele.
B) DNA sequences of WT AIP (bottom) and of the mutated allele (top). N.B. the two 9 base-pair long repeats, the 5’ one marked in purple (caaggcctac) and the 3’ one marked in blue (caaggcccac). The duplicated sequence (italic) introduces additional amino acids in the protein binding domain TPR3.
C) Cartoon representation of the atomic structure of AIP, highlighting the two pairs of helices forming the TPR2 (light orange) and TPR3 protein binding domains.
D) Close up of structures mediating binding between WT AIP and HSP90 (blue peptide) and simulation of the effect of the seven amino-acid AIP duplication (purple) on the AIP structure mediating HSP90 binding. Residue K266 (green), in the wild-type AIP interacts with the HSP90 peptide (or with TOMM20 peptide). From Salvatori EJE 2017.
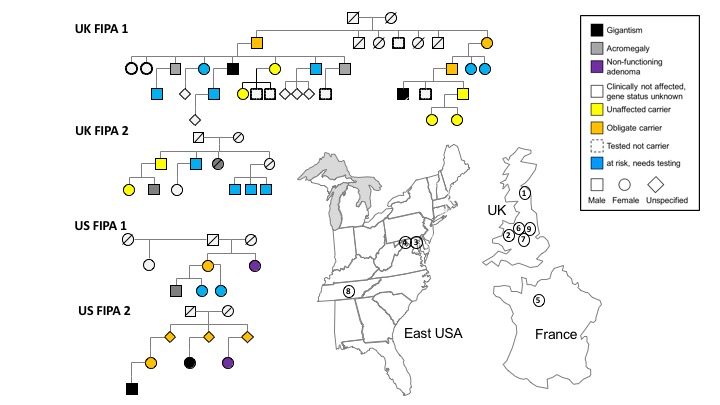
Figure 4. Pedigrees of the English founder AIP c.805_825dup (p.F269_H275dup) mutation and geographical locations. From Salvatori EJE 2017.
Recent research projects
Hormone effects and metabolism
 Nearly one percent of the general population and 2.5% of those above 70 years of age are on long-term glucocorticoid treatment for a chronic inflammatory disease. Many of these patients develop iatrogenic Cushing syndrome, causing significant metabolic, cardiovascular and musculoskeletal morbidity for which there is a treatment need but no current solution. We conducted a clinical trial exploring a concept arisen from our previous experimental studies (Christ-Crain, Faseb J, 2008, Pubmed 18198220 and Kola JCEM, 2008, Pubmed 18782871): many of the changes seen in glucocorticoid excess correspond to metabolic steps regulated by the enzyme 5’AMP-activated protein kinase (AMPK), a key regulator of energy metabolism and one of the well-recognized mediators of metformin’s mode of action (Pernicova & Korbonits, Nature Rev Endocrinal, 2014). We assessed the effect of metformin in glucocorticoid-treated patients. Despite the relatively short duration of the study, we found, in addition to glucose-related positive outcomes, beneficial effects in several cardiovascular, metabolic, bone and inflammatory parameters. Key findings with significant relevance to healthcare were the lower frequency of pneumonia in the metformin group compared with placebo, reduced overall rate of moderate-to-severe infections and, most significantly, lower all-cause hospital admissions.
Nearly one percent of the general population and 2.5% of those above 70 years of age are on long-term glucocorticoid treatment for a chronic inflammatory disease. Many of these patients develop iatrogenic Cushing syndrome, causing significant metabolic, cardiovascular and musculoskeletal morbidity for which there is a treatment need but no current solution. We conducted a clinical trial exploring a concept arisen from our previous experimental studies (Christ-Crain, Faseb J, 2008, Pubmed 18198220 and Kola JCEM, 2008, Pubmed 18782871): many of the changes seen in glucocorticoid excess correspond to metabolic steps regulated by the enzyme 5’AMP-activated protein kinase (AMPK), a key regulator of energy metabolism and one of the well-recognized mediators of metformin’s mode of action (Pernicova & Korbonits, Nature Rev Endocrinal, 2014). We assessed the effect of metformin in glucocorticoid-treated patients. Despite the relatively short duration of the study, we found, in addition to glucose-related positive outcomes, beneficial effects in several cardiovascular, metabolic, bone and inflammatory parameters. Key findings with significant relevance to healthcare were the lower frequency of pneumonia in the metformin group compared with placebo, reduced overall rate of moderate-to-severe infections and, most significantly, lower all-cause hospital admissions.
Our data could have immediate clinical relevance as the simple treatment suggestion – metformin treatment for patients on glucocorticoid treatment, even if they do not have diabetes. The results leading to clinically relevant significant impact on a large number of patients on long-term glucocorticoids via improving their treatment-related complications and cardiovascular prognosis. Although there are a large number of patients treated with glucocorticoids in the UK, Europe and US, there is increasing use of biologics or other steroid-sparing agents. However, other parts of the world still rely heavily on glucocorticoids. A safe, cheap and effective prevention/treatment of major metabolic complications of long-term glucocorticoid use is eagerly awaited, and our study showed that metformin could be served as a treatment. The data has been published in Lancet Diabetes and Endocrinology with an accompanying editorial: Metformin: the white knight fighting corticosteroid side-effects.
Pernicova, I., Kelly, S., Ajodha, S., Sahdev, A., Bestwick, J.P., Gabrovska, P., Akanle, O., Ajjan, R., Kola, B., Stadler, M., Fraser, W., Christ-Crain, M., Grossman, A.B., Pitzalis, C. & Korbonits, M. Metformin to reduce metabolic complications and inflammation in patients on systemic glucocorticoid therapy: a randomised, double-blind, placebo-controlled, proof-of-concept, phase 2 trial. Lancet Diabetes and Endocrinology 2020; 8: 278-291. ^10.1016/S2213-8587(20)30021-8
Download: Metformin: the white knight fighting corticosteroid side effects, Reincke Lancet D&E 2020 Comment [PDF 130KB]
Media coverage: Daily diabetes pill which costs just 15p could end the dreaded 'moon face' side effect of steroid medication which causes the face to swell up, Daily Mail, 14 March 2020
Schematic representation of how AIP deficiency leads to the aggressive phenotype in AIPpos tumours
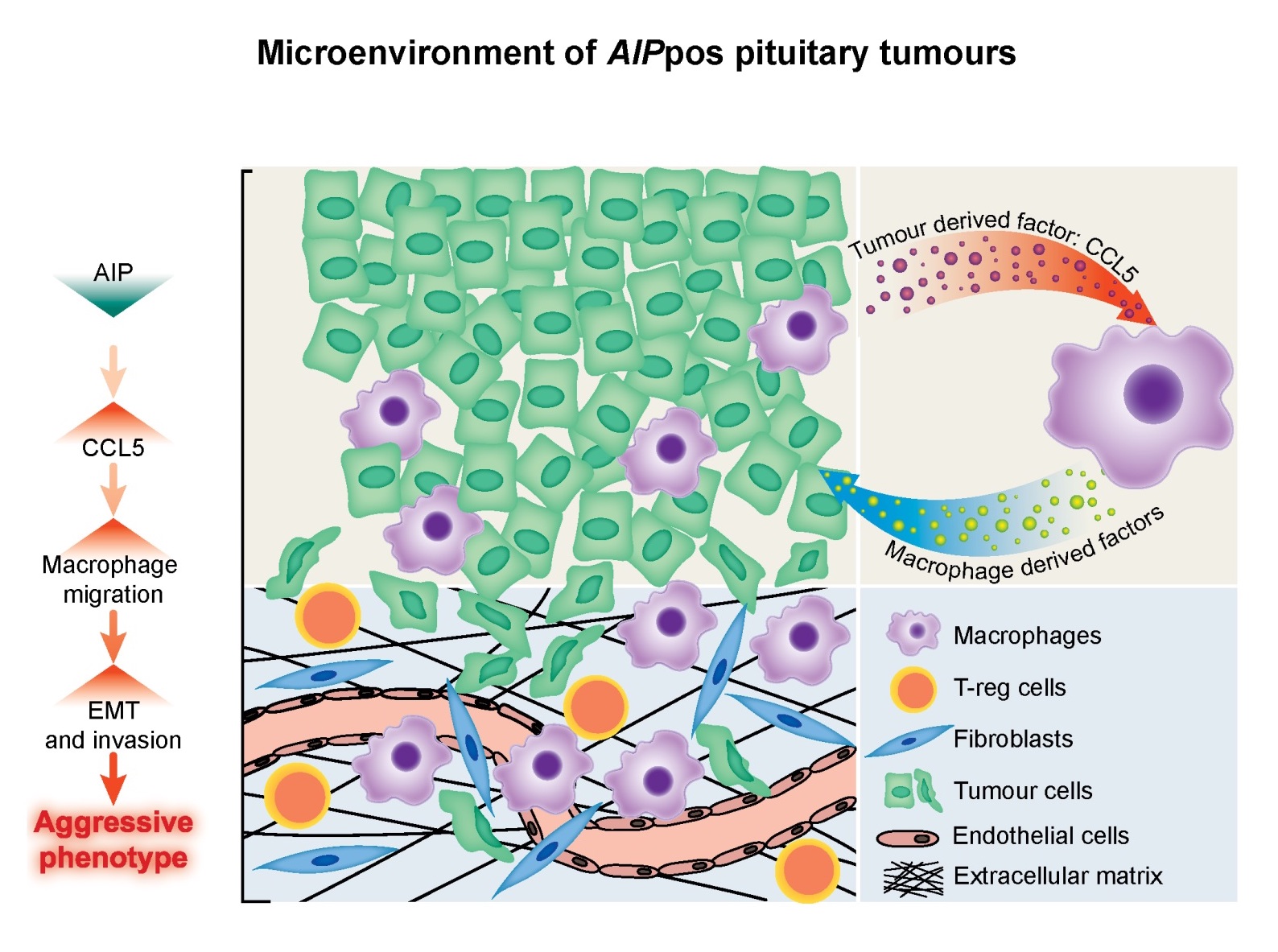 Crosstalk between AIPpos tumours and the tumour microenvironment. AIPpos tumours have EMT signatures and increased immune cell contents, cytokines and abundant vascular structures which create a tumour supportive microenvironment to promote aggressive tumour growth. The upregulation of the CCL5 in the AIPpos tumours and the in vitro data presented suggest that CCL5, secreted by the tumour cells, may contribute to the recruitment of macrophages and initiate bidirectional paracrine signalling loops which facilitate increased migratory/invasive potential of the tumour cells. Our findings indicate that AIP deficiency in pituitary cells drives invasion through the induction of EMT and immune cells recruitment.
Crosstalk between AIPpos tumours and the tumour microenvironment. AIPpos tumours have EMT signatures and increased immune cell contents, cytokines and abundant vascular structures which create a tumour supportive microenvironment to promote aggressive tumour growth. The upregulation of the CCL5 in the AIPpos tumours and the in vitro data presented suggest that CCL5, secreted by the tumour cells, may contribute to the recruitment of macrophages and initiate bidirectional paracrine signalling loops which facilitate increased migratory/invasive potential of the tumour cells. Our findings indicate that AIP deficiency in pituitary cells drives invasion through the induction of EMT and immune cells recruitment.
The tumour microenvironment of pituitary tumours
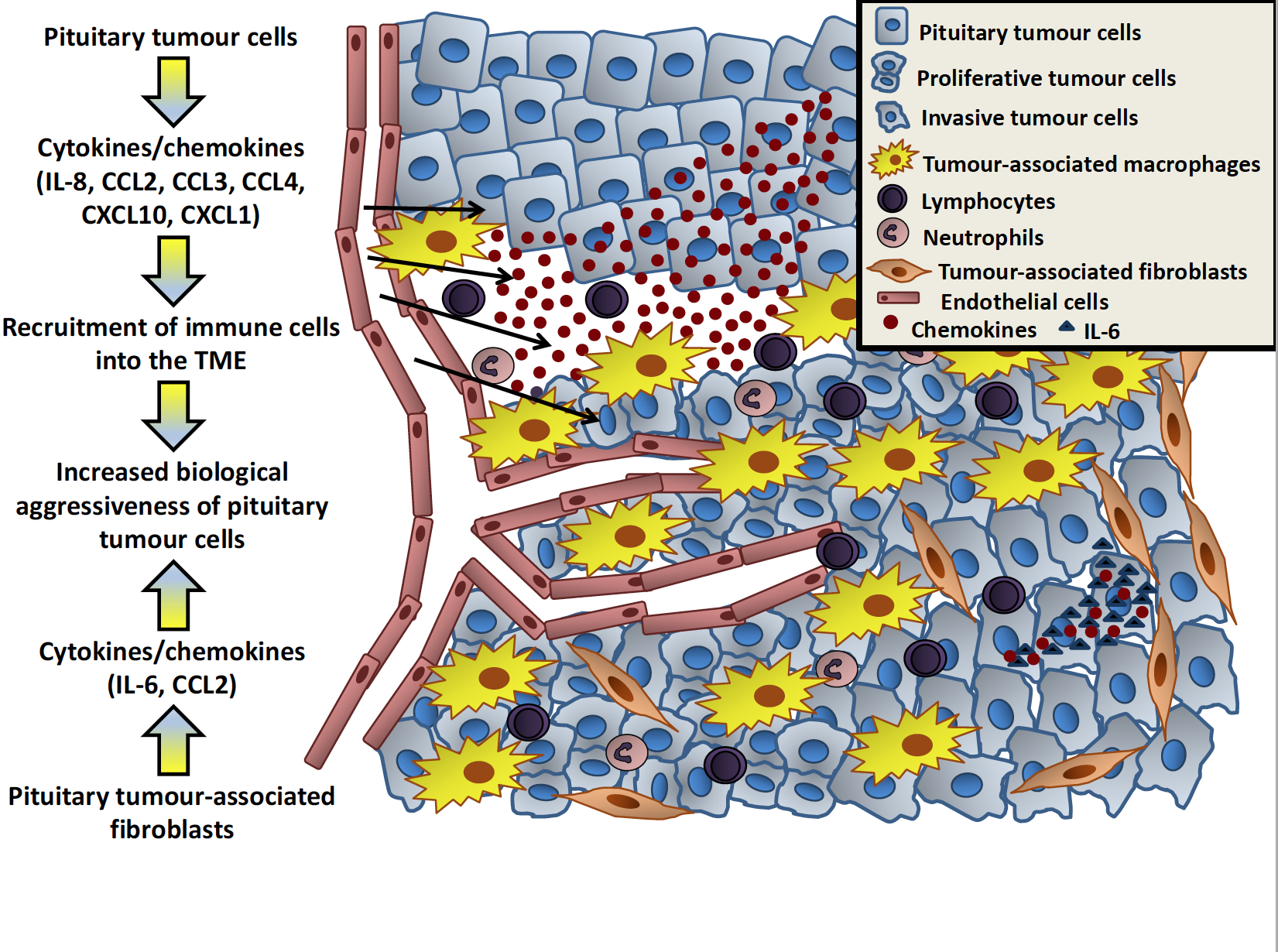 Pituitary tumour cells release different cytokines, particularly chemokines (including IL-8, CCL2, CCL3, CCL4, CXCL10, CXCL1), directly into the tumour microenvironment promoting the recruitment and infiltration of immune cells, including macrophages, lymphocytes and neutrophils. These infiltrating immune cells increase the growth of the tumour. Fibroblasts within the tumour are also able to secrete cytokines, such as IL-6, into the tumour microenvironment, which leads to increased invasion of pituitary tumour cells or the surrounding tissues.
Pituitary tumour cells release different cytokines, particularly chemokines (including IL-8, CCL2, CCL3, CCL4, CXCL10, CXCL1), directly into the tumour microenvironment promoting the recruitment and infiltration of immune cells, including macrophages, lymphocytes and neutrophils. These infiltrating immune cells increase the growth of the tumour. Fibroblasts within the tumour are also able to secrete cytokines, such as IL-6, into the tumour microenvironment, which leads to increased invasion of pituitary tumour cells or the surrounding tissues.
Marques, P., Barry, S., Carlsen, E. et al. Chemokines modulate the tumour microenvironment in pituitary neuroendocrine tumours. acta neuropathol commun 7, 172 2019. https://doi.org/10.1186/s40478-019-0830-3 Marques, P., Barry, S., Carlsen, E. et al. Pituitary tumour fibroblast-derived cytokines influence tumour aggressiveness, Endocrine-Related Cancer, 26, 12 2019. https://doi.org/10.1530/ERC-19-0327
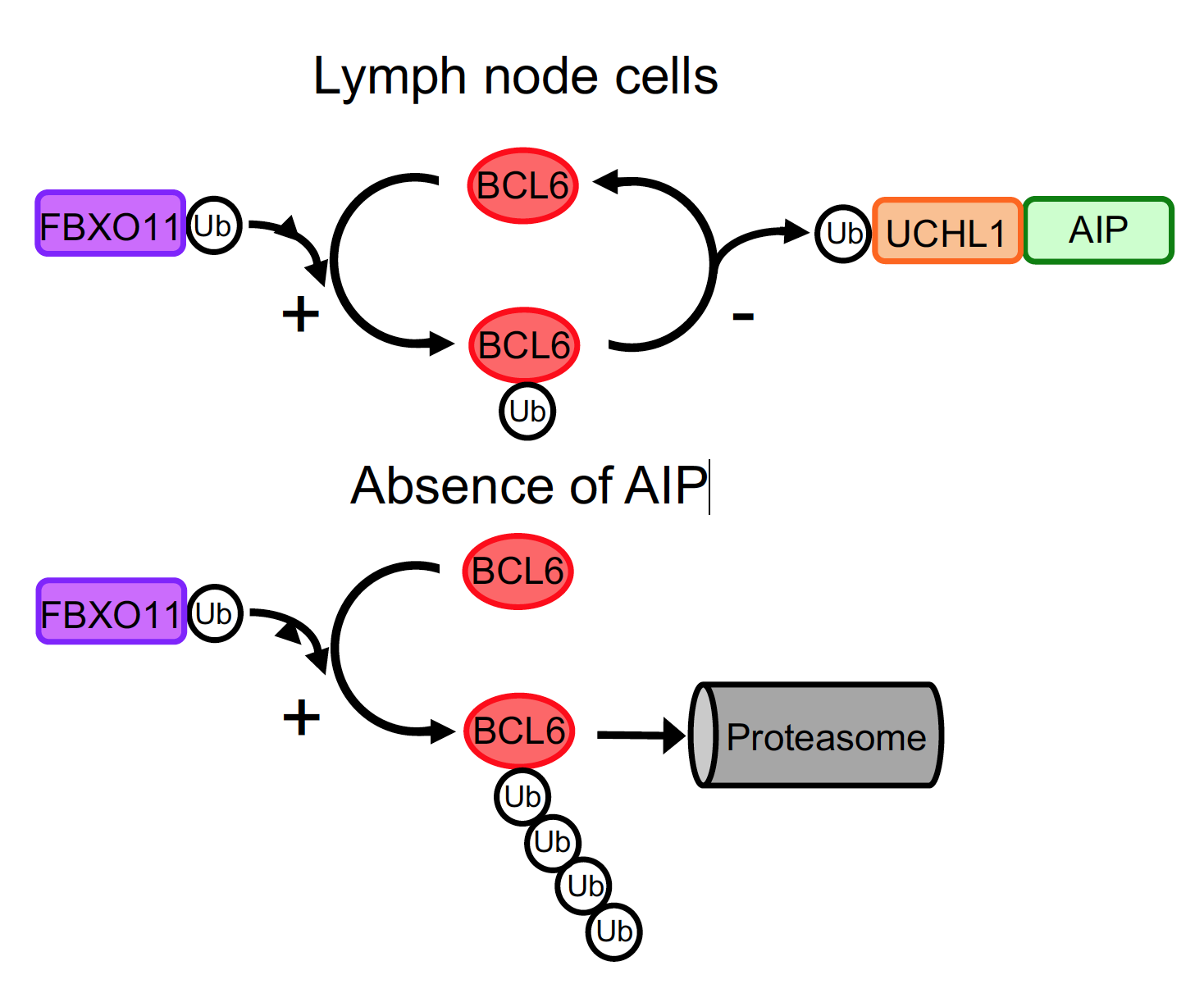
BCL6 – protein supporting lymphoma growth FBXO11 – protein attached ubiquitin chain to BCL6 Ub- ubiquitin molecules forming a chain UCLH1 – protein which cuts off ubiquitin chain from BCL6 Proteasome - the cell system to degrade proteins
AIP - the bad guy
While in pituitary tumours AIP seem to be fending off cancer, in lymphoma (a certain type of blood cancer) AIP seems to support those cells which generate cancerous growth. BCL6, a protein supporting cell proliferation and AIP are both highly expressed in a certain type of lymphoma (Diffuse Large B cell Lymphoma). Proteins get degraded if a particular molecule-chain (ubiquitin-chain) is attached to them and escape degradation if this chain is cut-off. We found that AIP supports the enzyme which cuts off the ubiquitin-chain from BCL6. Lack of AIP results increased amount on ubiquitin-chain associated BCL6 which then results in BCL6 degradation. This new mechanism could be exploited in the treatment of B-cell lymphoma.
Sun, D., Stopka-Farooqui, U., Barry, S., Aksoy, E., Parsonage, G., Vossenkamper, A., Capasso, M., Wan, X., Norris, S., Marshall, J.L., Clear, A., Gribben, J., MacDonald, T.T., Buckley, C.D., Korbonits, M. & Haworth, O. Aryl hydrocarbon receptor interacting protein maintains germinal center B cells through suppression of BCL6 degradation [PDF 4,781KB]. Cell Reports 2019; 27: 1461-1471 e1464. ^10.1016/j.celrep.2019.04.014
